Representation Ready: A Design Checklist for AI Healthcare Imagery
When Paid, But Not Portrayed went live, my inbox filled up with two main reactions.
Midlife Black women and other women of color wrote, “Yes, this is exactly what I see in HeyGen and Kling. Thank you for saying it out loud.”
Product teams and healthcare marketers wrote a different question.
They asked, “Okay, so what does good look like? What does representation ready actually mean if we want to use AI images in women’s health and menopause campaigns without causing more harm?”
That is the work of this piece.
I am a Black, board-certified surgeon turned menopause physician and neuroaesthetic creative director. I build campaigns, patient education, and media systems that live at the intersection of hormones, nervous systems, and pixels.
So when I say “representation ready,” I am not talking about a diverse stock photo slapped on a landing page. I am talking about visuals that can sit in front of a real woman at 2 a.m. when she is searching “night sweats menopause” on her phone and her nervous system is already tired.
Representation ready is a safety feature, not a decorative add-on.
Why AI healthcare imagery is never neutral
Every image is already a kind of clinical note.
Before a woman reads a single word on a page, her body is scanning the visual field for:
- Whose body is here
- How old she looks
- What color and texture her skin and hair carry
- Whether this scene feels like the world she lives in or a world she has to squeeze herself into
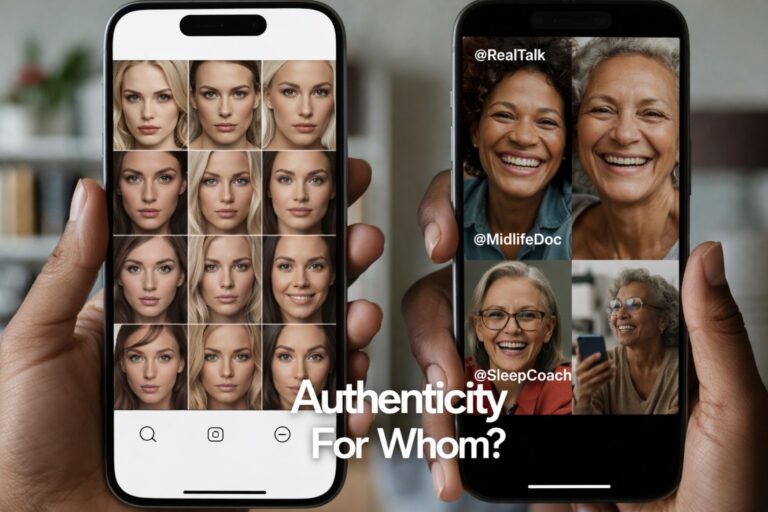
If your AI tool only offers thin, under 40, mostly white-presenting bodies, it is not just an aesthetic choice. It is a sorting mechanism. It tells some viewers, “You are the default patient we had in mind.” It tells others, “You are an exception we will get to later, if at all.”
That sorting has consequences in menopause and midlife health, where Black women and other women of color already face:
- delayed diagnosis
- more severe symptoms
- higher burden of cardiovascular and metabolic risk
- a long history of being unseen or disbelieved
When AI systems inherit that same narrow palette and call it “user friendly,” they carry those patterns forward into the digital front door of care.
Three common failure patterns in AI healthcare imagery
Across image tools, avatar platforms, and stock-style generators, I see the same repeating problems.
1. Youth and whiteness as the silent default
The library is full of:
- young women in their twenties and early thirties
- a smooth range of hair colors and outfits
- minor tweaks in features, all orbiting the same narrow ideal
As soon as you:
- age the subject past 45
- deepen the skin tone
- ask for natural hair textures or protective styles
the output quality drops or the variety disappears.
The tool is not “bad at older Black women.” The tool was never truly trained for them.
2. Diversity as costume, not continuity
Some platforms will show one or two “diverse” images on their homepage.
Inside the interface, that variety collapses. You get a handful of token faces that have to carry an entire spectrum of race, culture, and region. They feel like costumes, not people with lives.
In a menopause campaign, that shows up as:
- one ambiguous brown woman used in every slide about “inclusion”
- no visual continuity between campaign images and the community it is meant to reach
- a nervous system sense of “this looks like marketing, not like my auntie or my neighbor”
3. Clinical implausibility
Health content has an extra layer of responsibility.
I often see images that are technically impressive but clinically off:
- postmenopausal topics illustrated with women who look 28
- “hot flash” visuals that show heavy makeup and flawless styling rather than the reality of a flushed, sweaty, tired face
- hospital or clinic scenes that ignore real dress codes, demographics, or body types
The result is a strange friction. The words say “we see you.” The images say, “We are talking to someone else.”
What “representation ready” actually means
Representation ready is my short way of saying:
This visual system has enough range, integrity, and context that real women can see themselves in it without having to translate or shrink.
For AI healthcare imagery, representation ready requires five layers.
1. People: range of age, race, body, and role
A representation ready library for menopause and women’s health should include:
- Age range: women in their 40s, 50s, 60s and beyond, not just “timeless 30s”
- Racial and ethnic range: multiple Black women, Latinas, Asian and Pacific Islander women, Indigenous women, multiracial women, white women, each with more than one face
- Body diversity: varied sizes, heights, and proportions without caricature
- Role diversity: patients, clinicians, caregivers, founders, workers, not just “beautiful woman as model”
If you can count the number of midlife Black women in your library on one hand, you are not representation ready.
2. Context: believable environments
The background matters as much as the face.
Ask:
- Does this exam room or office look like a place my audience actually receives care?
- Are tools, clothing, and spaces consistent with real-life practice, not just generic “medical” vibes?
- For remote care content, do the home scenes reflect a range of socioeconomic realities?
Representation is not only who is in the frame. It is also where they are allowed to exist.
3. Aesthetic and sensory safety
From a neuroaesthetic perspective, imagery for health and menopause education should:
- avoid over-smoothing and over-glossing that make skin look plastic
- show natural lines, pores, gray hair, and texture with respect
- use color palettes that support regulation rather than jolt the nervous system
We are not trying to create clinical horror or glam perfection. We are trying to make it easier for a woman’s body to say, “I can stay with this information.”
4. Voice and narrative alignment
The visual should match the story you are telling.
If your copy is about:
- nervous system overwhelm
- medical gaslighting
- reclaiming body trust in menopause
and the image looks like a generic tech ad, your audience feels the mismatch.
Representation ready visuals reinforce the narrative instead of competing with it.
5. Process: how the images are chosen and maintained
This is where a lot of teams fall short.
A representation ready process includes:
- having diverse clinicians, patients, and community voices involved in reviewing visuals
- building feedback channels so users can flag images that feel off or harmful
- setting explicit targets for age and race range instead of hoping “the model will learn”
Without process, good intentions decay over product cycles.
The Representation Ready checklist for AI healthcare imagery
You can use this as a preflight checklist before publishing any AI-generated campaign, landing page, or educational asset.
People
- At least three age bands are visible (40s, 50s, 60s plus).
- Multiple midlife Black women and women of color appear across the materials, not just once.
- Body shapes and sizes vary in realistic ways.
- Women appear in more than one role: patient, clinician, leader, friend, caregiver.
Context
- Environments feel like real clinics, homes, offices, or digital spaces your audience uses.
- Details such as clothing, equipment, and room layouts are plausible.
- There is no reliance on vague “healthcare blue” backgrounds alone.
Aesthetic and sensory safety
- Skin looks like skin, not plastic. Texture and aging are present without ridicule.
- Color choices support legibility and calm attention.
- No images lean into stereotypes or aesthetic trauma for effect.
Narrative alignment
- The people in the image could believably be saying the words in your copy.
- Visuals and text point to the same audience and life stage.
- Campaigns for menopause and midlife do not use exclusively under 40 models.
Process and accountability
- Someone on the team has explicit responsibility for representation integrity.
- There is a way for patients, users, or partners to give feedback on imagery.
- You can name at least one concrete change you made after listening.
If you cannot check most of these boxes, you are not in trouble. You are simply not done.
How teams can start implementing this today
You do not need a giant budget or a full rebrand to begin.
1. Audit one campaign
Pick one live or upcoming campaign in women’s health or menopause and perform a simple audit:
- Count how many images show midlife or older adults.
- Count how many clearly Black, brown, and Indigenous women appear.
- Note where the visuals feel disconnected from the copy.
Use those observations to decide what must change before launch.
2. Rewrite your AI prompts
Most prompts stop at “diverse middle aged woman” and hope the model does the rest.
Try prompts more like:
“Midlife Black woman physician, age 52, natural hair, in a teal blazer, sitting at a desk reviewing menopause lab results with a patient on a laptop, warm natural light, realistic skin texture.”
Specificity is not a luxury. It is how we retrain the machine.
3. Build a mini advisory circle
You do not need a thirty person council.
Invite:
- one clinician of color who works in midlife health
- one patient or community advocate
- one designer or creative
Ask them to look at a small set of images and give you honest feedback. Listen without defending.
4. Partner where you lack capacity
Not every organization can hold all of this in house.
Studios like Ceyise exist because there is a growing need for AI-guided creative direction that understands both the clinical landscape and the cultural stakes.
If you are selling tools into menopause, women’s health, or neuroaffirming care, representation ready is not optional. It is part of your risk management.
This is about future viability, not just optics
We are heading into a world where AI will be able to generate “authentic looking” content in any aesthetic you request. What will distinguish the tools and teams that last is not raw image fidelity.
It will be whether real humans inside real bodies can look at your work and say:
- “I recognize myself here.”
- “This feels like it was built with me in mind, not added for optics.”
- “I can trust the people behind these pixels enough to keep reading, keep watching, keep engaging.”
Midlife women are not edge cases. We are not an afterthought. We are clinicians, founders, caregivers, partners, and patients. We are paying for these tools and using them to teach and heal.
If your AI healthcare imagery cannot hold us in its frame with integrity, your system is not representation ready. And if you are willing to do the work to change that, you are the kind of team I want building the next generation of tools.